Africa has made great strides over the past decade in providing life-saving treatment to HIV patients. But there is a new and growing danger that these advances might not be sustained, owing to high demand and dwindling financial support.
NEW YORK – At Uganda’s largest AIDS clinic, I recently witnessed a remarkable celebration of life. The performers were a troupe of young African singers, drummers and dancers, ranging in age from roughly eight to 28. Rarely have I been so profoundly moved.
“This is a land,” they sang,
“Where beautiful people
Laugh and dance in harmony.
Africa. O Africa.”
And, indeed, these young people laughed and danced not only in harmony but with a joie de vivre that lit up their faces and filled us all with happiness. Listening, it was hard to imagine that they could easily be dead – and would be, if not for this clinic.
Access every new PS commentary, our entire On Point suite of subscriber-exclusive content – including Longer Reads, Insider Interviews, Big Picture/Big Question, and Say More – and the full PS archive.
Subscribe Now
Each of those splendid performers is living with HIV. Some arrived at the clinic so ill that they could scarcely walk. Others showed few symptoms but, having tested positive, came to be treated. They were mothers and fathers, sisters and brothers, children and grandparents. All were alive and healthy for one reason only: the Joint Clinical Research Center in Kampala, and the drugs that it provides them.
Uganda was the epicenter of the AIDS epidemic. There the scourge began in earnest; there (as elsewhere in Africa) it exacts its highest toll. Yet Uganda is also a success story. A decade ago, fewer than 10,000 people were taking the new generation of antiretroviral drugs that suppress the disease and offer the promise of a normal life. Today, that figure is 200,000, thanks in large measure to generous support from the United States (under its PEPFAR program) and the Global Fund in Geneva.
We have seen similarly encouraging progress elsewhere. Botswana, among others, has invested heavily to offer universal treatment, and now is well on its way to ensuring that no baby is born with HIV – a reality in developed countries, but not so in Africa, where 400,000 children are born with the disease each year. South Africa, with the largest number of people living with HIV, has spent nearly $1 billion over the past year in an ambitious counseling and testing campaign to roll back the epidemic.
But there is a new and growing danger that these advances might not be sustained. Peter Mugyenyi, who runs the Joint Clinical Research Center, told me that part of the problem is the sheer weight of numbers. In Uganda, only about half of those with HIV/AIDS are being treated. Meanwhile, money for treatment is drying up. Because of the global recession, some international donors are threatening to cap their financial support.
Countries such as Malawi, Zimbabwe, and Kenya, as well as Uganda, are requesting assistance for emergency drug supplies. In Kampala, Dr. Mugyenyi has begun placing new patients on a waiting list. As many as seven million Africans who should be getting treatment for HIV are not. Worldwide, the number is about 10 million.
Compounding the problem: donors have also been shifting their focus from AIDS to other diseases, because there is a sense that more lives can be saved more cheaply. At a time when we should be scaling up to meet the AIDS challenge, we are dialing back. In our global war on AIDS, the international community is on the verge of snatching defeat from the jaws of victory.
Those who rallied to the fight are alarmed. They fear that the impressive gains of the last decade will be lost. “We are sitting on a time bomb,” Dr. Mugyenyi told me. Every day, he is forced into moral choices that no one should have to make. How do you choose to treat a young girl but not her little brother? How do you turn away a pregnant mother, sitting with her children, crying for help?
Surely we can do better. In Kampala, I promised my young friends that I would do everything I could to help. In Washington recently, the United Nations rolled out an action plan that should dramatically accelerate progress on maternal and child health, including HIV. At the International AIDS Conference in Vienna, in July, I hope that the international community will rally around UNAIDS’ launch of Treatment 2.0 — the next generation of HIV treatment, which must be more affordable, more effective, and accessible to all.
As chair of this year’s replenishment of the Global Fund, I urge all donors to see to it that countries such as Uganda get the support they need, so that Dr. Mugyenyi and other front-line soldiers in the fight against AIDS need not make those difficult choices.
I left Uganda with a snatch of song that still echoes within my heart. Its inherent truth would be obvious, had you been there to see:
We are still useful.
To our countries, to our families.
All we need is a way to live our days,
All we need is to survive in Africa.
Yes, times are hard. That is all the more reason to act out of compassion and with generosity.
To have unlimited access to our content including in-depth commentaries, book reviews, exclusive interviews, PS OnPoint and PS The Big Picture, please subscribe
By trying to running the state like a private business, Elon Musk and other anti-government types are creating a mess that someone else will have to clean up. Governments and businesses serve vastly different purposes, answer to different constituencies, and operate on entirely different timelines.
explain why ongoing efforts to run the state like a business are doomed to fail.
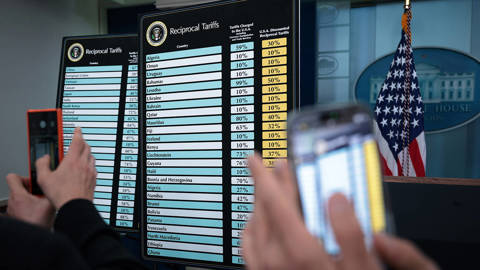
US President Donald Trump says he wants to preserve the dollar's international role as a reserve and payment currency. If that's true, the history of pound sterling suggests he should be promoting financial stability, limiting the use of tariffs, and strengthening America's geopolitical alliances.
applies three lessons from prewar Britain that the Trump administration appears determined to ignore.








NEW YORK – At Uganda’s largest AIDS clinic, I recently witnessed a remarkable celebration of life. The performers were a troupe of young African singers, drummers and dancers, ranging in age from roughly eight to 28. Rarely have I been so profoundly moved.
“This is a land,” they sang,
“Where beautiful people
Laugh and dance in harmony.
Africa. O Africa.”
And, indeed, these young people laughed and danced not only in harmony but with a joie de vivre that lit up their faces and filled us all with happiness. Listening, it was hard to imagine that they could easily be dead – and would be, if not for this clinic.
Introductory Offer: Save 30% on PS Digital
Access every new PS commentary, our entire On Point suite of subscriber-exclusive content – including Longer Reads, Insider Interviews, Big Picture/Big Question, and Say More – and the full PS archive.
Subscribe Now
Each of those splendid performers is living with HIV. Some arrived at the clinic so ill that they could scarcely walk. Others showed few symptoms but, having tested positive, came to be treated. They were mothers and fathers, sisters and brothers, children and grandparents. All were alive and healthy for one reason only: the Joint Clinical Research Center in Kampala, and the drugs that it provides them.
Uganda was the epicenter of the AIDS epidemic. There the scourge began in earnest; there (as elsewhere in Africa) it exacts its highest toll. Yet Uganda is also a success story. A decade ago, fewer than 10,000 people were taking the new generation of antiretroviral drugs that suppress the disease and offer the promise of a normal life. Today, that figure is 200,000, thanks in large measure to generous support from the United States (under its PEPFAR program) and the Global Fund in Geneva.
We have seen similarly encouraging progress elsewhere. Botswana, among others, has invested heavily to offer universal treatment, and now is well on its way to ensuring that no baby is born with HIV – a reality in developed countries, but not so in Africa, where 400,000 children are born with the disease each year. South Africa, with the largest number of people living with HIV, has spent nearly $1 billion over the past year in an ambitious counseling and testing campaign to roll back the epidemic.
But there is a new and growing danger that these advances might not be sustained. Peter Mugyenyi, who runs the Joint Clinical Research Center, told me that part of the problem is the sheer weight of numbers. In Uganda, only about half of those with HIV/AIDS are being treated. Meanwhile, money for treatment is drying up. Because of the global recession, some international donors are threatening to cap their financial support.
Countries such as Malawi, Zimbabwe, and Kenya, as well as Uganda, are requesting assistance for emergency drug supplies. In Kampala, Dr. Mugyenyi has begun placing new patients on a waiting list. As many as seven million Africans who should be getting treatment for HIV are not. Worldwide, the number is about 10 million.
Compounding the problem: donors have also been shifting their focus from AIDS to other diseases, because there is a sense that more lives can be saved more cheaply. At a time when we should be scaling up to meet the AIDS challenge, we are dialing back. In our global war on AIDS, the international community is on the verge of snatching defeat from the jaws of victory.
Those who rallied to the fight are alarmed. They fear that the impressive gains of the last decade will be lost. “We are sitting on a time bomb,” Dr. Mugyenyi told me. Every day, he is forced into moral choices that no one should have to make. How do you choose to treat a young girl but not her little brother? How do you turn away a pregnant mother, sitting with her children, crying for help?
Surely we can do better. In Kampala, I promised my young friends that I would do everything I could to help. In Washington recently, the United Nations rolled out an action plan that should dramatically accelerate progress on maternal and child health, including HIV. At the International AIDS Conference in Vienna, in July, I hope that the international community will rally around UNAIDS’ launch of Treatment 2.0 — the next generation of HIV treatment, which must be more affordable, more effective, and accessible to all.
As chair of this year’s replenishment of the Global Fund, I urge all donors to see to it that countries such as Uganda get the support they need, so that Dr. Mugyenyi and other front-line soldiers in the fight against AIDS need not make those difficult choices.
I left Uganda with a snatch of song that still echoes within my heart. Its inherent truth would be obvious, had you been there to see:
We are still useful.
To our countries, to our families.
All we need is a way to live our days,
All we need is to survive in Africa.
Yes, times are hard. That is all the more reason to act out of compassion and with generosity.